The IOM: Death by Acronym and Epic Media Fail
Background
The illness myalgic encephalomyelitis (ME) has probably existed for centuries. It has been documented since an occurrence in Los Angeles, California in 1934, followed by countless other similar events. A major outbreak at the Royal Free Hospital in London, UK in 1955 led to the coining of the term “myalgic encephalomyelitis”.
In 1988 the term “chronic fatigue syndrome” (CFS) was created in the US; this generally replaced ME in many countries, including the UK. However, the trivialising nature of the name CFS was deeply unpopular with most patients so the terms have frequently – but misleadingly – become conflated, either to ME/CFS or CFS/ME. I have lived with ME since 1981. There is still no cure nor any approved treatment. It is a global illness with a long and troubled history everywhere.
************
The latest chapter
In 2013 the Institute of Medicine (IOM – renamed the National Academy of Medicine in 2016) was tasked by the US Department of Health and Human Services (HHS) with researching and developing new diagnostic criteria/clinical definition, considering new terminology and proposing an outreach strategy for their dissemination.
The resulting 300-odd page report was presented on 10 February 2015 in Washington, DC (with a 54-minute video). It received widespread media coverage – more than 300 articles and stories, according to patient organisation Solve ME/CFS Initiative (as of 14 Feb) – which began to emerge at 11.01am, one minute after the meeting began.
Embargoed press information was clearly circulated in advance to selected media outlets and journalists. However, this information was unavailable to the recognised cohort of serious patient bloggers and advocates; those representing many of the 20 million or so patients worldwide who live with this illness were, as always, responding off the back foot. If my deduction is correct, then we are still in an era of control rather than collaboration. If patient are not key stakeholders in this process then I don’t know who is.
In the UK, there has been limited media interest so far; the Mail online carried the story, while the BMJ and New Scientist have articles behind paywalls. Articles from other countries also started to trickle through.
The media coverage
Most of the reporting which I have seen could best be described as vanilla. A brief mention of the background to the illness is coupled with two main themes: that this is a real and serious illness and now we have a new name. Muted hurrahs all round, punctuated with an occasional harrumph. But this is not the real story; the real story is the scandal of an entire patient population which has been marginalised, stigmatised and wilfully neglected for generations. The fact that the IOM, along with other agencies (the NIH’s P2P is next up), has recently been charged with addressing that appalling deficit is an insidious distraction from that deeply unpalatable core issue.
During the presentation, chair of the IOM’s committee, Dr Ellen Wright Clayton, said that the report gives advocates and patients a “tool” with which to “act up“. No, Dr Clayton, we are the ones who are ill and we’ve been doing this for far too long. Besides, the situation for patients with HIV/AIDS was – and continues to be – very different from that of ME patients. The way in which we are still treated by government agencies in all countries is a scandal – and always has been. Until that is publicly and universally acknowledged, we cannot move forward, however noble your stated intentions. The time for a complete top-down culture shift is way overdue. I may be a UK citizen but what you do affects me too. We have had enough.
The devil in the detail
Patients everywhere responded rapidly with their comments, mostly via blogs and social media. These – along with the broader media commentary – dissected the detail (good and bad) and provided close analyses of the minutiae of the report. And I, too, have some carefully considered remarks:-
Report: (cue fanfare) Our proposed new diagnostic criteria:
->Me: Huh?
Report: …..and we suggest a new ICD-10 coding.
->Me: The European ICD-11 beta draft went online in 2012 but good luck with that.
Report: You’ll like this; there’ll be a new toolkit!
->Me: Kill me now.
Report: We say new criteria need to be disseminated and used by clinicians for this to work.
->Me: Well – duh.
Report: And we need to improve awareness and education about this disease.
->Me: Again – du-uuh.
Report: More research and funding is needed into this dreadful disease.
->Me: And again….. (you get the picture)
Report: We propose a new name. Yay! “SYSTEMIC EXERTION INTOLERANCE DISEASE – S.E.I.D”.
->Me: W.T.F?
Cost: One million dollars.
A note on the proposed new name
“Systemic” – means generally affects the whole body. Um – yes.
“Exertion intolerance” – at this point I see an ethereal Victorian lady with a fit of the vapours, having foolishly attempted to bestir herself from her chaise longue (no doubt in order to retrieve her copy of Freud’s latest blockbuster). Great image for patients already long stigmatised as the lazy, crazy people.
“Disease” – well I’ll get on board with that one but what changed? Patients have been wanting this for decades but were advised that there wasn’t enough evidence to support such a label. Did someone put something in the water at the IOM?
“ME” sucks. “CFS” sucks. “ME/CFS” and “CFS/ME” suck. “SEID” sucks. They all suck. Probably best left alone until we’ve focused on the research. With realistic funding. And a patient-led, pro-active media/lobbying strategy, in which the patient community controls its own agenda (see previous post.) A counter-balance to the current bland mainstream reporting.
************
What happens now?
This report needs to be accepted by HHS and other agencies before it becomes effective; however, it seems likely that the recommendations will be adopted. At that point, it will be interesting to see how far its impact extends into other countries.
In fairness, the report contains some excellent work which could bode well for the future. The IOM committee members undertook a very challenging task. Many patients have welcomed the recommendations and believe that they emphasise the urgent need for action and will accelerate the speed of change. Arguably, one of the most pressing needs of the international patient community is hope; if the report achieves this, then it will have improved the lives of some. However, a less charitable observer might conclude that we have heard these platitudes too many times before and that anything of value here is several decades too late.
Whatever happens next is certainly too late for the millions of patients who have already died during the last eighty years. Most of them never had their illness validated nor were they treated with respect and compassion in their lifetimes. And what assurance is there that anything concrete will happen during the next thirty years? Another generation of us – including me – will have died before then. That sucks.
************
If you have been affected by any of the issues raised in this post, then please call A.A. (Acronymics Anonymous) immediately. Acronyms can be fatal.
The Secret Files Unwrapped: Part I – the importance of fair and accurate records (with file download)
 Introduction
Introduction
I created this blog in August 2012 to publish my investigations into the so-called “Secret files on ME”. It was set up rather hurriedly in order to counteract some misinformation which was circulating at the time. My work was not finished when I started the blog and it took me some time to complete the process. In the absence of any proper treatment for myalgic encephalomyelitis or ME (also known, unhelpfully, as “chronic fatigue syndrome” or CFS), my health continues to deteriorate and my progress is painfully slow.
The full story of my work on getting these files opened up is set out in a post from November 2012. This is a brief summary of the background to the files, taken from that post (edited for clarity):
For several years, there had been considerable speculation and rumour surrounding some “secret” files on ME (the illness I have lived with since 1981) which are held in The National Archives (TNA) at Kew in London, UK. In September 2011 I used the Freedom of Information Act of 2000 (FOIA) to see if the files could be opened up.
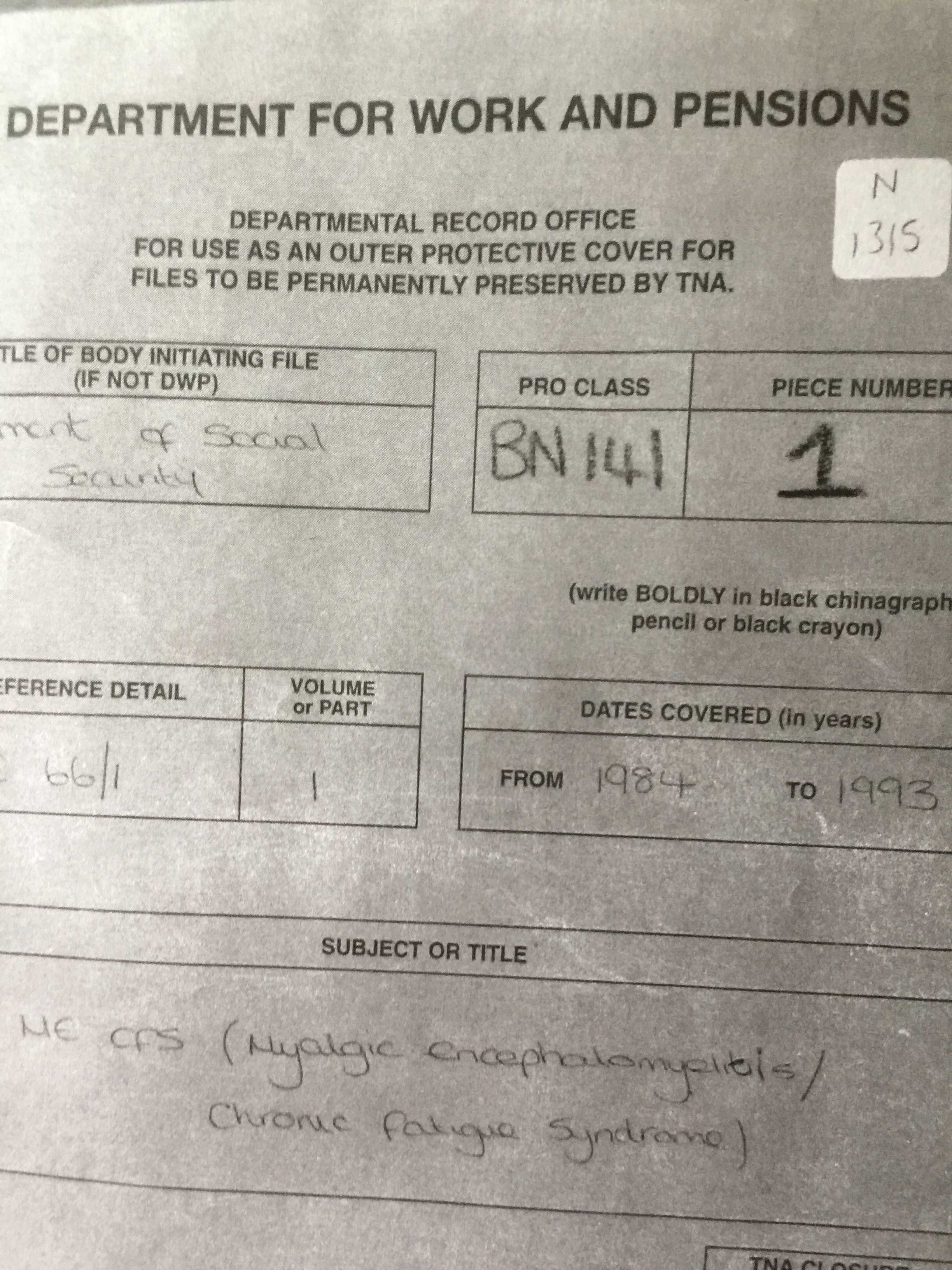
It transpired that there were two files – one from the Department of Work and Pensions (DWP, formerly known as the Department of Social Security – DSS) and one from the Medical Research Council (MRC). The files contain documentation about ME (correspondence, notes of meetings, background material and details of benefits claims/research applications). Both files had been reviewed and archived in the normal way during the 1990’s.
Both files contained information which was properly exempt from disclosure under the Freedom of Information Act. They were therefore closed to the public until 2072 (DWP – pictured above left) and 2071 (MRC).
NB. this process had nothing to do with the Official Secrets Act. The files were neither classified nor secret. They simply contained confidential information.
As a result of my work, both files are now available (although still with some unavoidable redactions). The DWP file can be downloaded by scrolling down to the bottom of this post and following the link. The MRC file can be downloaded from the next post in this series at this link here.
It was always my intention to upload the files here as soon as I was able. Both files can be found elsewhere online but not everyone who has an interest will necessarily have been able to access them. My aim is to make them more widely available for academic, educational and research purposes. They stand in their own right as historical records relating to the formulation of UK policy on ME/CFS (sic) during the 1980’s and 1990’s. Accurate historical records play a crucial role in every democratic society.
To the best of my knowledge, no official record exists which truthfully documents patients’ experience of living with ME. The illness itself has been documented since the 1934 Los Angeles outbreak in the US. It was accurately described by doctors following the “Royal Free disease” outbreak in the UK in 1955. Nearly a hundred years on, despite the existence of these, and many other, records, the real nature of the illness is still denied by many doctors, either actively or simply by default. Patients are still stigmatised and abused; the illness is still not properly recognised, the result being that there are still no officially-approved treatments available anywhere which actually treat the condition and address its wide range of symptoms.
************
The complete absence of a visible patient narrative became painfully evident last week. The British media’s wilfully ignorant coverage of ME patients’ perceived “fear of exercise” gave the headline writers a field day (examples here and here).
Many journalists simply regurgitated a press release from the Science Media Centre’s relentless propaganda machine, having failed to make any responsible enquiry into the real story. Subsequent rebuttals from patient groups and charities limped in on the back foot. Inevitably, however, the positive and corrective commentary was drowned out in the general furore. Patients and supporters rallied but were all too late to the party.
Why? How could this happen yet again? Because it can. Because that real story, patients’ actual lived experience, is invisible. It remains unseen and largely undocumented. Accounts of individual patients’ experiences appear occasionally, often in local media or comment sections of national media, but their impact is low. At worst, these stories may even serve to normalise the shocking way in which patients are treated and the illness portrayed, rather than exposing the underlying scandal.
Chronically sick ME patients are not up to the herculean task of funding, developing and managing a long overdue strategic initiative and media campaign in order to disseminate the real story pro-actively and counter negative publicity. But without such a campaign in place, it will happen again. The ME community remains without a credible platform from which to speak and generate an accurate record for the archives.
Do media stories really matter? Yes, of course they do – because those stories are subsumed into the source materials which constitute our collective history. If there can be no aggregation of fair and accurate records, then history is falsely written and becomes a mere propaganda tool.
************
So – back to those files, which form part of the UK’s official record of ME policy development and remain, so far, officially unchallenged. Reading them is a deeply distressing experience. In an effort to minimise the impact on my health of writing this post, I have not re-read them recently. I’m therefore posting them without further discussion. Both files are quite long so I am going to spread them over two posts. Both still contain redacted portions for reasons which are explained in my original post (see link in second paragraph of this post).
The link at the foot of this post is for the DWP file (previously the Department of Social Security – DSS). It is 235 pages long and is described as follows on the title page on TNA’s website: “Medical policy formulation; consultation with medical experts and advice from Board of Doctors“. The illness is described as “ME CFS (Myalgic Encephalomyelitis/Chronic Fatigue Syndrome)” and the dates covered are 1984-1993.
There are two ways of viewing this file. One is to visit TNA at Kew in south-west London and view the original; the other is to look at the photographic version of the file in the link below. Taking photographs of 235 already rather blurry pages was a laborious process and unfortunately the image quality is not the best. However, I hope that readers will be able to garner the information they need. I will upload the other file (the MRC file) in Part 2 of this post.
***********************
TO DOWNLOAD the DWP pdf image FILE (this may take a few minutes so please be patient):
Click on LINK HERE NatArchBN141DSS
Karina Hansen 1: Prisoner of Denmark
 IMPORTANT UPDATE 2016
IMPORTANT UPDATE 2016
This post is quite old and does not contain much detail about the background to Karina’s story. For newer and more in-depth analyses of Karina’s situation, the entire series can be viewed as a whole at the Karina Hansen series category section of this blog and particularly note Karina Hansen 6: The HOMECOMING
********************
Many readers will already be aware of the case of Karina Hansen. However, for those of you who are unfamiliar with her situation, this is a short re-cap of the facts as far as we know:
Karina (pictured above left), now aged 25, is a citizen of Denmark, a member state of the European Union. She was diagnosed in 2008 with a severe case of the illness myalgic encephalomyelitis or ME (also known, unhelpfully, as chronic fatigue syndrome or CFS). Her family cared for her at home until February 2013 when state intervention caused her to be forcibly removed to the Hammel Neurocenter for mandatory treatment as a de facto psychiatric patient. Despite the efforts of her family, friends and the international ME/CFS patient community to secure her release and return home, she has remained there ever since. The British charity Invest in ME has offered advice and assistance to the Danish authorities but has, so far, been ignored.
**********************
In the last year, Karina’s case has been taken up by Danish physician Dr Stig Gerdes. Dr Gerdes has challenged the whole concept of Functional Disorders and, in particular, how this notion has been used to psychologise Karina’s original diagnosis of ME (something with which most ME patients – including me – will be all too familiar). Dr Per Fink who is in charge of Karina’s treatment at the Hammel Neurocenter, has been robustly defending himself against Dr Gerdes’ comments. An example of Dr Fink’s approach can be found here. It makes for chilling reading (the first couple of pages are enough to get the picture).
The debate between the two doctors has now descended into Dr Fink referring Dr Gerdes to the Danish Medical Ethics Board. Recent correspondence between them has been released by Dr Gerdes on this FB page (the name of which translates as “Caught in the Municipal System”) https://www.facebook.com/IKlemmeIDetKommunaleSystem in a post dated 27 June 2014 (you may need a translation tool, as my link shows as “translation unavailable” but Google/Bing works well enough).
Unfortunately, the effect of this professional dispute is simply to deflect attention away from the real issue at the heart of this case which is the inappropriate medical treatment and enforced detention of a seriously ill young woman. For a more detailed account of the background to this case see this excellent blog post. It is from last year but the position has not changed substantially since then. [Note: unfortunately, Karina’s situation is far from being the only one of its kind. There are a number of similar cases worldwide involving both adults and children. This has been the position ever since this illness began to be documented in the 1930’s. However, that discussion is beyond the scope of this post].
Renewal of Karina’s state-appointed guardian
As is normal in such cases, Karina was assigned a state-appointed guardian to ostensibly represent her interests. On 25 June this year, the question of his re-appointment was considered by the court. The campaigning group Justice for Karina Hansen requested that members of the patient community send emails to the court to express their concern, with a copy to the Minister for Health. This is a valuable campaigning strategy although, for legal reasons, the emails will not have been considered in the court’s deliberations. In the event, Karina’s guardian was re-appointed until 22 September when there will be another court hearing. This the text of the email which I sent:
I have followed the case of Karina Hansen since her detention at the Hammel Neurocenter in February 2013. I understand that the renewal of the appointment of her guardian is due before the court on 25 June.It is difficult to understand from the outside exactly what is happening as there is only a very limited amount of information available. However, from a medical perspective, Ms Hansen does not appear to be receiving appropriate medical treatment for her originally diagnosed condition of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS).From a legal perspective, it would appear that the actions of the Danish state might be in breach of various provisions of the European Convention on Human Rights and the Charter of Fundamental Rights of the European Union.These are matters of grave concern to the international ME/CFS patient community. I would suggest that Ms Hansen’s guardian has not fulfilled his obligations and duties and therefore his re-appointment may not be in Ms Hansen’s best interests.I understand that, as an individual, I have no locus in the court hearing regarding Ms Hansen’s guardianship. Nevertheless, it is important that an expression of concern for the circumstances of this case can be publicly made to all the relevant parties.Thank you for your attention.Valerie Eliot SmithUK lawyer and ME patient since 1981
Karina is no longer at Hammel Neurocenter, but has been moved to Tagdækkervej, a different facility in Hammel……This new facility is within walking distance from Hammel Neurocenter. It is a facility where patients with different health issues live in small apartments for privacy, but have access to rehabilitation facilities and staff from Hammel Neurocenter. This facility has a special focus on patients with various brain injuries, but other patients are accepted.
Page v Smith explained
Following my previous post about the controversial case of Page v Smith [1995] UKHL 7 , I decided it might be a good idea to draft a simplified version of what actually happened in the case.

The scales of justice
Let’s start with a quick re-cap of the facts of the case:
In 1987, Mr Page and Mr Smith were involved in a minor road traffic accident which, it was agreed, was the fault of Mr Smith. Mr Page sustained no direct physical injury from the accident but did suffer a major relapse of his myalgic encephalomyelitis (ME – also sometimes known, unhelpfully, as chronic fatigue syndrome or CFS) and so he claimed damages from Mr Smith. The case went all the way up to the House of Lords (which in 2009 became known as the Supreme Court). The House of Lords (HL) found in Mr Page’s favour, although not unanimously. The Law Lords remitted the matter back down to the Court of Appeal for a final determination. The Court of Appeal, having found against Mr Page the first time around, now found in his favour – in 1996.
So, in the interests of clarity, I have come up with this explanation.
PAGE v SMITH – THE ALTERNATIVE VERSION
High Court: Nice judge. Lots of jolly good but largely irrelevant [“obiter“] discussion about ME (real illness; nasty business). Didn’t like The Weasel*. Secretly felt sorry for Mr P so awarded damages.
Court of Appeal (1): Nasty lot. Lots of squabbling. Couldn’t make up their minds so they took Mr P’s money away and buggered off to the pub.
House of Lords: More judges. More squabbling. P has ME; P has accident; P suffers “nervous shock” [an archaic legal term] caused by accident; nervous shock causes a “recognisable psychiatric illness” (bit wobbly about exactly what illness because we’re only pretend doctors and PTSD is still in beta at the moment); said illness triggers relapse of ME. Bingo. My judgment’s bigger than yours.
Court of Appeal (2): Back again FFS. Last lot buggered off to the pub and forgot to determine causation. Of course the accident made Mr P worse. Give the man his money back and get those bloody insurance companies out of here. Mine’s a G & T. Obiter.
Case comment by Mr Page and Mr Smith: Dude – nine years. Seriously?
***************************
Anyone fancy doing the rap version?
* Pejorative name for an expert witness in the case.
Turning the Page (and the Smith): checking the facts – and why we need to broaden the debate
NOTE: for the short version of this post see the next post Page v Smith Explained
This has been a difficult post to write for reasons which will become apparent. I drafted it several days ago but have been debating since then whether or not to go ahead with it. I’ve now decided that, however difficult it is on a personal level, there is a much broader public interest in raising these issues.
***************************
The world of cyberspace is an unimaginably vast store of information. Some of it is excellent, some of it rather less so, some is misleading and the rest pretty much defies acceptable description. Anyone with internet access now has a route into this huge repository which was previously inaccessible; this resource is, on balance, a great gift to all of us. However, it is not always easy to process that information into useful and practical knowledge.
The illness known as myalgic encephalomyelitis or ME (also sometimes known, unhelpfully, as chronic fatigue syndrome or CFS or ME/CFS) is no exception to this rule. There is an article which is currently (March 2014) doing the rounds within the ME community. A few people have asked me for my view on it so I’m offering my observations here. The article appeared recently on an ME website and is entitled “ME/CFS is an organic disorder“. I should make it clear that I have great respect for the author’s work in general but, in my opinion, there are some problems with this particular piece. However, I would not have written this post had I not specifically been asked for my view.
NB. Before finalising this post, I contacted the website’s manager a few days ago and expressed my specific concerns regarding the article. As a result of our communications, one minor alteration was made but otherwise it appears to retain its original text.
Most of the article deals with the series of judgments in the case of Page v Smith (Page v Smith [1995] UKHL 7) , from the mid-1990’s. These were the facts of the case:
In 1987, Mr Page and Mr Smith were involved in a minor road traffic accident which, it was agreed, was the fault of Mr Smith. Mr Page sustained no physical injury as a direct result of the accident but did suffer a major relapse of his ME and so he claimed damages from Mr Smith. The case went all the way up to the House of Lords (which in 2009 became known as the Supreme Court). The House of Lords (HL) found in Mr Page’s favour, although not unanimously. The Law Lords remitted the matter back down to the Court of Appeal for a final determination. The Court of Appeal, having found against Mr Page the first time around, now found in his favour – in 1996.
This was a protracted and complex case. The important points arising from it in the context of its significance to ME patients/advocates are these:
- This is a personal injury (PI) case in which the main legal issues are causation (how the injury was caused), foreseeability and nervous shock.
- For nervous shock to succeed in a claim for damages, it must result “in some recognisable psychiatric illness” (see para 3 of Lord Keith’s judgment in the HL decision).
- Although ME occupied a large proportion of the discussion and certain findings were made, it was not specifically about ME.
- The comments made by the various judges about the nature of ME as a condition are therefore peripheral (“obiter“, in legalese), not central, to the issues.
- Those comments are not legally binding, nor are they medically significant. They were made purely in the context of deciding this case on its particular facts.
- While this is an important PI case, it is from twenty years ago and has been much criticised. The correctness of the decision was doubted in a 2010 article in the Cambridge Law Journal [1]
It is therefore not correct to say “it is enshrined in English case law that ME/CFS is a physical, not psychiatric, disorder although the mechanism by which a relapse may occur following trauma is via nervous shock“. Medical evidence is also required showing a consequential “recognisable psychiatric illness” which, as the Court found in Mr Page’s case, then triggered a relapse of the ME symptoms. That is how he got his damages – via a psychiatric route. This was not a “landmark” case about ME, nor was it a helpful decision.
Obtaining transcripts of judgments
This is often a laborious process, even for practising lawyers/academics and where the case is recent. However, I retrieved the House of Lords judgment in Page v Smith without too much difficulty. The link is in that case reference and above and it is available to anyone. The first instance decision (Page v Smith [1993] PIQR Q55) and the second Court of Appeal judgment (Page v Smith (No 2) [1996] 3 All ER 272-280) were only accessible to me via my academic route so I cannot provide links here as they won’t work.
If you have the correct references, all recorded cases in English law are available. However, access may be limited because they are 1) behind a paywall 2) require an academic/judicial status or 3) necessitate a visit to an old-fashioned law library. This is mainly because digitisation of all recorded cases only became standard within the last ten years. Out-of-court settlements of damages (which are frequent in PI cases) are not recorded judgments.
“Gagging orders”
These are more correctly known as confidentiality agreements or non-disclosure agreements (NDA’s). They are not uncommon in cases which involve awards of damages. While they may not be desirable in terms of public transparency, they can serve a legitimate purpose. It does not appear that there was such an agreement in Mr Page’s case. (Gagging orders may also be imposed by a court via an injunction).
***************************
The use of misleading information assists no one – and that includes us as ME patients/advocates. Using incorrect information to support our arguments only helps those who seek to discredit us as ill-informed or deluded conspiracy theorists. It is better that we focus our limited energies on cultivating more robust arguments using the wealth of more accurate information which is readily available.
We need all the tools at our disposal to achieve proper recognition, research and treatment for ME. Whilst we certainly need to know and understand the history of the illness, we also need to focus our efforts on collecting and utilizing accurate and up-to-date information in our advocacy work.
We need to broaden the debate, both internally and externally. Within the ME community, we need to learn how to read and analyse more critically and to engage respectfully in conversations which are founded on disagreement. Conflict and confrontation are inevitable but the less we actively provoke it (or over-react to it), the better. If we cannot do this, then our detractors will continue to retain the upper hand. Ensuring that our information is accurate and not misleading is an essential part of that process.
****************************
Brief update on the Wikipedia topic (see previous post)
I’m grateful to everyone who responded, both publicly and privately, regarding the Wikipedia issue in my last post. I learnt a great deal from all your comments.
I think it’s fair to say it’s unlikely that anyone will be making a serious attempt to update the CFS page (or adding an ME page) any time soon. It’s a sad state of affairs – but one that is all too common in the world of ME patients.
*******************************************
Footnote:
[1] Stephen Bailey (Professor of Public Law at the University of Nottingham) and Donal Nolan (Porjes Foundation Fellow and Tutor in Law at Worcester College, University of Oxford) concluded a comprehensively critical legal article on Page as a PI decision in the Cambridge Law Journal in 2010 as follows:
For anyone with access to internet legal providers such as Westlaw or LexisNexis or to a law library, the citation is CLJ 2010 (69)3, 495 – 528.The Scottish Law Commission has proposed that the foreseeability aspect of Page be overturned by legislation, and argued that in determining the foreseeability of psychiatric injury an assumption of reasonable fortitude should ordinarily be used. And although the [English] Law Commission in its report on this area did not make a similar recommendation, it said that it appreciated the concerns raised by the critics of Page, and pointed out that at the time of its report insufficient time had passed to assess the impact of the decision. The most likely mechanism of reform is the Supreme Court, and here the omens look favourable. In the two recent decisions of the House of Lords which touched on Page there was a distinct lack of enthusiasm for the decision. In Rothwell, Lord Hope described the argument that the foreseeability aspect of Page should be departed from as “attractive”, while preferring to “leave it for another day”. Lord Mance also left open the correctness of the decision “for another day”. He saw some force in the criticisms that had been levelled against Page and was not confident that it did not cause uncertainty and argument. And while Lord Hoffmann expressed the view that it would not be right to depart from Page, this was only because it did not appear to have caused any practical difficulties and was not likely to do so if confined to the kind of situation which the majority in the case had had in mind. Furthermore, in Corr v. IBC Vehicles Ltd, Lord Neuberger said that, not least in the light of the “trenchant observations” of Lord Goff in White, he would not want to appear to prejudge any decision as to the correctness of the decision in Page if it came to be challenged before the House on another occasion, comments with which Lord Mance expressed his agreement. Taken together, these remarks would suggest that it may not be long before the Page v. Smith saga finally reaches its denouement.
Lean in*: the IOM, Wikipedia and a bit more legal
“About”
I have recently updated and expanded the About section of this blog for the benefit of both new and existing readers. Please feel free to visit it for more information.
***************************
The Institute of Medicine’s (IOM’s) Committee for Diagnostic Criteria for “ME/CFS” – Public Information-gathering Session, 27 January 2014, Washington, DC (NB. the IOM was renamed the National Academy of Medicine in 2016)
The controversial background to the recent tasking of the IOM by the US Department of Health and Human Services (HHS) to create a new definition of myalgic encephalomyelitis/ME (often conflated unhelpfully with chronic fatigue syndrome/CFS) is very ably described in this blog post by Erica Verrillo Briefly, the process by which this took place appeared excessively rushed and lacking transparency.
The ME patient community has generally speaking been deeply concerned by this for several reasons:
- There are already two good case definitions available in the Canadian Consensus Criteria and the International Consensus Criteria, both of which are acceptable to most patients and ME expert practitioners (but not, it would seem, by state institutions), therefore:-
- The IOM contract is wasting US$1 million. This is about 20% of the paltry $5 million budget assigned to this illness. Apparently male-pattern baldness gets $18 million (thanks to Dr Nancy Klimas for that little gem).
- Clinical case definition is not a normal part of the IOM’s remit. The only other example of which I am aware was their astonishing result with Gulf War Illness (GWI) in 2013, a complex condition with many similarities to ME. The IOM’s new definition? “Chronic multi-symptom illness”. The outraged Gulf War veterans are now desperately engaged in trying to unscramble that disaster.
One half-day segment of the 2-day Committee meeting was the only part made available to the public. I watched the live webcast and was hoping that the videos would be made available by the time I published this post. [UPDATE: 2 hours after this post went live, they duly appeared here.] The meeting agenda is here.
The second half of the meeting was given over to presentations by ME patients/advocates (7) and members of the public (15) ie. more advocates, many of whom are living with the illness themselves. This makes their appearances (some live and some online) and the excellent quality of their presentations even more astounding.
I must stress that my observations are purely subjective and working from memory; my vantage point was limited to the scope of the fixed webcams in the room. However, two significant procedural aspects struck me as I watched the webcast. Firstly, that the spirit of the First Amendment (similar to Article 10 of the European Convention on Human Rights) seemed to have been firmly locked out of the room. The proceedings appeared rigidly-controlled and exclusionary.
Secondly, the atmosphere in the room felt sterile, devoid of empathy and compassion. I watched a few appalling moments (as, I’m sure, did many others) as a wheelchair-bound presenter struggled to take her place at the table (she couldn’t reach the podium), trying to move obstructions and set up her presentation kit with no external assistance. At that point, other patient-advocates rushed from their places (at the outside edges of the room) to help her and she eventually overcame the patently disabled-unfriendly environment.
The patients/advocates leaned in with great courage and dignity. However, in spite of lip service to the contrary (see Dr Nancy Lee’s remarks here), they seemed to be unwelcome and unheard (there were very few questions from the Committee members). Does a constitutional right to freedom of expression have any meaning in the absence of a subsidiary right to be listened to by the state which should be upholding those rights?
So why does this meeting matter for anyone outside the US?
Because what happens in the US will have a profound knock-on effect on the global ME community, no matter where we live. Because the US has a large community of exceptionally active and eloquent patients/advocates. Because, over the last half-century, we have learnt to our cost that the definition of a disease will dictate its perception, research, diagnosis and treatment. Because we are all connected.
It’s pretty much open season for conspiracy theorists now.
**************************
Some of the advocates have been generous enough to make texts of their presentations available via websites and blogs. I appreciate that there is a lot of reading here but even by looking at just one you will probably learn something you didn’t know before. I did. The saddest thing of all is that almost everything you will read here has been repeated over and over again for many years and yet we still have no appropriate model for dealing with ME in any country in the world.
The presentation links below are alphabetical by name. There are differences between their approaches but I would not endorse any one above the others. I have nothing but admiration and gratitude for everyone who spent their precious time, money and energy preparing for and attending this meeting.
Derek Enlander (delivered by Jay Spero)
Phoenix Rising (website statement)
Maryann Spurgin (delivered by Charlotte von Salis)
NOTE: As far as I can make out, everything in these links has already been made available to the public. It was not feasible for me to contact everyone individually for clearance to post. However, if any of the people named above object to the inclusion of their statements, then please contact me (see “About” for details) and I will remove it.
*************************
Wikipedia; the importance of definitions. Who will take up the challenge?
Dr Leonard Jason reminded us of the importance of naming in his recent (short) blog post “Diseases can stigmatize” . In my previous post, I mentioned that I had a problem with using Wikipedia as a reference for ME/CFS because, if you enter “Myalgic Encephalomyelitis” into its search box, you are automatically redirected to “Chronic Fatigue Syndrome“. This was never acceptable. But, of course, as one commenter pointed out recently, “Wikipedia is editable”.
[EDIT: June 2025 The Wikipedia page has now been updated. I don’t know when this took place as it’s some time since I last checked it but the new version, while still not ideal, is a significant improvement. The updated page can be viewed here.]
There have been unsuccessful attempts by patients in the past to edit the Wikipedia “chronic fatigue syndrome” entry. I think the time has come again for someone else to give it another go (or perhaps someone recently has and has a story to tell about the experience?). This is not a challenge which I could take up as I do not have either the medical or technical expertise which would be required to make a proper attempt. However, if anyone would like to give it a go then I would love to hear about it in due course.
A word of caution: I think it would need a team of at least two people, preferably one person with the requisite medical knowledge and one with technical/Wiki experience so that they can give it their best shot. It could take some time but, if properly pursued, the result could be either a proper stand-alone “myalgic encephalomyelitis” entry on the internet’s greatest information resource or a documented account of how it was impossible to create a legitimate entry for this much-maligned illness.
This action would create a platform for the matter to then be formally be raised with Wikipedia and generate media interest but, for that to work, it must be as professional and watertight as possible. Please note: I do not intend to orchestrate this challenge; I simply throw it out in case anyone wants to run with it.
NOTE: the person who made the previous Wiki-attempt might be willing to provide some background information but doesn’t wish to be actively involved in trying again. I can supply further details if anyone wants to pursue this further.
*************************
Legal loose ends
I’m conscious that in previous posts, I have mentioned the possibility of legal routes to further the cause of proper recognition for ME patients and their illness. I have dealt with this issue in a fairly perfunctory fashion as it is a huge and complex area. It is a matter which is constantly in the back of my mind but which I am unlikely to have the energy to explore here in the foreseeable future.
However, for those who are interested, I would draw your attention to the excellent UK Human Rights Blog which explains in simple language the process of Human Rights litigation in countries which have signed up to the European Convention on Human Rights. While HR legislation is only one component of the mechanism which might be used to challenge the state on the rights of ME patients, it is nevertheless an important and fascinating area.
*************************
Walking like an Egyptian in 2014
It’s exactly a year since I last wrote anything for this blog. I didn’t mean to leave it this long but I’ve just been too ill to write. I have had plenty of ideas and thoughts which I wanted to write about but it just hasn’t been possible. I don’t yet know whether or not I will be able to start writing more regularly again; my health has been very bad during the last year but I’m hoping that there is a slight improvement now.
For any new readers, I have lived with the complex neuroimmune disease Myalgic Encephalomyelitis (ME) since 1981, in widely-varying degrees of severity. ME is also known – very unhelpfully – as chronic fatigue syndrome (CFS). At this point, I usually provide a link to the Wikipedia entry for those who want to know more about the illness but I’m not going to do that this time. If you put “Myalgic Encephalomyelitis” into Wikipedia you go automatically to “chronic fatigue syndrome”. There is no stand-alone entry for ME; this is symptomatic of the nightmare of this illness. Even the name is disputed, let alone its classification, diagnostic criteria and ultimately its very existence, despite an estimated 20 million patients worldwide. However, for anyone who is looking for a more accurate definition, the International Consensus Criteria give a realistic overview of the symptoms of this disease (and, crucially, does NOT include simple “fatigue” – one of the greatest misnomers of all time). Most commentators habitually confuse fatigue with a state of having systemically low energy. Every human being experiences the former; far fewer people experience the latter, usually as an inevitable consequence of chronic illness.
Blog update
The New Year brought a standard update from WordPress about my blog statistics, cheerfully trumpeting the fact that I’ve had a very modest 1100 views in the last year! Actually, for a blog that’s been dormant for 12 months, I’m very heartened by that. The total number of views topped 4000 (from over 50 different countries) just before the Christmas holiday period. By most standards, that’s pretty minimal but I’m actually delighted with that figure. The blog contained only 10 posts over a 6-month period so I reckon 4000+ views is pretty good going.
The original purpose of this blog was to disseminate information which I had gathered about the so-called “Secret” files on ME (see earlier posts in the sidebar from August and November 2012). That purpose remains and I will keep the blog live as a community resource, even if I can’t update it any further. I plan to do a review of the situation regarding the files but that will be (hopefully) in another post. I need to do some more research and updating to complete that task and I don’t have the strength to do it at the moment.
Despite being more disabled by the illness in the last year, I still monitor/research developments in ME and work on building networks with other patients. I receive occasional requests for assistance and I always respond and help wherever I can and will continue to do so. I spend much of my time working on relevant issues but because of my cognitive impairment (caused by the combination of long-term ME, too many anaesthetics and the inevitable ageing process) my progress is painfully slow and very limited in its scope. However, despite keeping rather quiet, I am still here and as committed as ever to the collective cause of bringing about change for the global ME community.
Brief review
A short round-up of current issues which I think merit highlighting; I would like it to be much more extensive but again, my resources will not permit that.
There is encouraging work taking place all over the world by both highly-respected medical institutions and by deeply-committed ME patients. Vast numbers of blogs and websites are constantly updating on developments in ME. I use many different resources (for example here, a post on cognitive problems which I find are the most distressing symptom of the illness). Each blog has its own agenda and there always will be people who don’t like what is said (as I know only too well); it’s simply a question of finding the resources which work best for you.
The community of patient-advocates in the US is, of necessity, particularly engaged and active at the moment. On the positive side, Jen Brea, who has severe ME, has just been interviewed by American Al-Jazeera TV ( Part 1 and Part 2 ) about her project Canary in a Coal Mine, a documentary film which she is making about the illness. On the negative side, the relevant US government agencies remain intent on treating the ME/CFS community with breathtaking arrogance and opacity. The story is far too complex for me to set out here but I do recommend Jennie Spotila’s blog which gives regular updates on its progress at Occupy M.E.
Continuing the good and the bad theme: the opening of the National Centre for Neuroimmunology and Emerging Diseases at Griffith University, Queensland, Australia, and its developing focus on ME/CFS, is a very positive step forward for the international community. Conversely, the detention of Danish citizen and ME patient Karina Hansen against her wishes and those of her parents continues to give cause for grave concern. Karina has been locked in a psychiatric facility for nearly a year. The lack of information is extraordinary; there may be legitimate legal reasons for this but I am baffled and appalled in equal measure by these events. I gather there are lawyers working on her behalf but what I cannot understand is how domestic and/or European law has not already provided a resolution to this shocking situation. However, the lack of information means that it is impossible to form a considered opinion on these events.
Fortunately for us, research continues on immunomodulatory and antiretroviral drugs (eg. Rituximab and Valganciclovir), gene expression, 2-day exercise testing as a diagnostic tool and many other areas – despite political apathy/obstruction and a significant lack of state funding/support. Again, many information sources are available.
Finally – the very bad: the controversy surrounding the completion in 2010 of the 5-year PACE Trial in the UK continues unabated. This trial was supposedly a demonstration that ME patients could benefit from a regime of Graded Exercise Therapy (GET) and Cognitive Behavioural Therapy (CBT). In other words, it further legitimized the most dangerous myths pertaining to this illness: that patients were not really ill, they only thought they were and therefore they could a) be brainwashed into thinking themselves well and b) remedy their deconditioning from inactivity with staged physical activity. Wrong on both counts. The Principal Investigators of this publicly-funded (£5m/US$8m) trial have repeatedly refused to release the full trial data; Queen Mary University of London is the relevant public authority which holds the information (Disclosure: I am a Visiting Scholar at QMUL). Those who continue to request this information under the Freedom of Information Act are frequently declared “vexatious” by the Information Rights Tribunal.
There are several important facts you need to know about the PACE Trial. Here are four of them:
- There is no internationally-agreed set of criteria for diagnosing ME (or CFS) so it’s quite possible that the trial included patients with other conditions (including psychiatric) or who didn’t have ME/CFS at all. There are multiple sets of criteria used across the world; the Oxford criteria were used for this trial in which fatigue can be a sole qualifying symptom.
- The most severely disabled patients were unable to take part – because they were too ill to even get to the hospitals, let alone take part in exercise
- The outcome measures were subjective – ie. mostly through self-reporting, a notoriously unreliable method of collecting data
- The outcome measures were “adjusted” during the course of the trial. It was possible to enter the trial with a score of 65 on the assessment scale (0-100, with 100 being someone in excellent health) and to finish with the lower score of 60 on the same scale but be counted as “recovered”. So a patient could enter with a score of 65, deteriorate to a level of 60 but still be counted as recovered within the trial parameters. (Incidentally, a score of 60 is similar to the level which a patient with congestive heart failure would be likely to achieve). Recovery? Seriously?
The sources for this information are multiple and I cannot list them all here. However, if anyone wants further information then I recommend this paper by patient-advocate Tom Kindlon (and many thanks to Tom for his assistance with the above) http://iacfsme.org/BULLETINFALL2011/Fall2011KindlonHarmsPaperABSTRACT/tabid/501/Default.aspx
Human Rights Question
I am often asked whether we should consider using European human rights law to challenge the status quo. Unfortunately, the short answer is that I don’t think it will help us for two reasons. First of all, it’s a very lengthy and time/energy-consuming process (ballpark – think 10 years and minimum £100,000/US$160,000). Secondly, and probably even more significantly, given the state of the current UK NICE guidelines, the argument which can be encapsulated as “The British healthcare system provides appropriate treatment according to the Guidelines, given the official current state of knowledge” would be likely to succeed. That’s not to say that it’s not worth a try (and it may be different in other countries, although I suspect the outcome would be similar) but, with those odds, it’s not really an option for most of us. There is also the problem of finding a competent and willing specialist lawyer. As I have already discovered, many reputable, high-profile lawyers (as with journalists and celebrities) don’t want to go anywhere near the controversy of ME issues. (That last statement opens up a whole other can of worms but I’m not going any further with that at this stage.)
Anatomy of a Successful Campaign
I’ve been putting off writing this section – partly because I’ve overstretched myself in writing this much (it’s already much longer than I intended) but also because it’s the most important issue for everyone who lives with this illness. If I do write further about this in due course, then I want to do it justice. ME has been in evidence for at least 150 years. It began to be recorded in several countries from the 1930’s onwards. In the UK, it has been properly-documented for over 60 years. That means that in the UK, for example, we are now seeing the emergence of the third generation of patients who are facing life with an illness which is still largely marginalised, ridiculed and untreatable. The earliest patients are mostly dead now, having had their lives invalidated by the prevailing culture and leaving only the heartbreaking legacy of their unheard voices.
Like most patients, I spend a disproportionate amount of time and energy trying to understand how this can possibly have happened and what might be the tool with which to dismantle the flawed medical/political/social constructs. It is a subject which demands greater research and consideration. I am right out of resources now but I hope to return to it at a later date. In the meantime, more patients will have died and Karina Hansen may still be incarcerated in her Danish prison. [update: Karina was finally allowed home in October 2016]
**************************************
Walking like an Egyptian in 2014
Ah yes – why this title? Well, the honest answer is that I wanted something catchy and this popped into my head from nowhere and wouldn’t go away. However, it occurred to me that it is, in fact, something I occasionally do in the middle of the night. To explain – like many people living with this disease, I sleep badly. I usually wake several times during the night, often in considerable pain and/or discomfort. Of necessity, I get up and walk around for a bit to ease the pain. My flat is constructed around a corridor with rooms off each side and I’m often to be found pacing up and down said corridor during the night. It can get a bit boring so I sometimes vary the steps a bit including – yes, walking like an Egyptian. So – next time you are wandering around with insomnia during the night, imagine me doing the same and perhaps we can start a trend. At least it might raise a collective smile in the loneliness of the wee small hours. (And in no way do I mean to minimise the current tragedy of democracy unravelling in the state of Egypt – but that’s a debate outside the scope of this blog.)
Thank you to everyone who has read this far. I send you my best wishes and hope to be back a bit sooner next time.
http://www.youtube.com/watch?v=Cv6tuzHUuuk&list=FLzbW98ow_XKOd5vlvPqULzA&index=3
The Shock of the New (Year): a Change of Direction
I’ve noticed that, after a certain age, New Year’s resolutions rather lose their appeal. However, the period of enforced merriment and un/happy families does require one to focus briefly outside the usual box. The ensuing return to normality can give a new perspective to old dilemmas. And behold – thus it was for me this time around.
It may have been apparent from my last post (in mid-December) that I needed to review my situation regarding how much work/writing I could continue doing. If I was in any doubt about how much I could do, the last few weeks have been uncompromisingly clear. My physical and emotional stress levels were high and this culminated in a severe relapse of my myalgic encephalomyelitis/ME symptoms. The pain was the worst I’ve experienced outside surgical situations and the level of weakness/neuropathic distress so extreme that, on one day recently, I was in a state of almost total physical paralysis. While this is not uncommon amongst patients with the most severe form of ME, mine is not usually quite that bad.
Inevitably, this recent episode has forced me to accept that I need to do things differently for the foreseeable future. The inescapable truth seems to be this: if I do anything else, I can’t write much. If I write regularly, I can do nothing else. There is so much I want to do that this leaves me pretty much stuck with the options of either 1) trying to maintain my blog and not achieving anything else or 2) pursuing my tentative plans for academic work/health campaigning but not blogging unless there is news of particular significance.
When I started drafting this current post, I discovered an abandoned draft from early December 2012 entitled “Four Levesons and a Funeral“. I was developing ideas for discussion over a range of issues. In the event, my energy levels have been so poor since then, that I had simply forgotten that I had even begun the draft.
*************************************
I never actually planned to start writing a blog. I set it up in August 2012 as a way of publicising my work on the “Secret Files on ME” (see posts from August and November 2012). My research was not complete at that time but there was some incorrect information about the files which was circulating on the internet. I needed to address this and so I responded by setting up this blog. Having started it, I wanted to preserve its momentum and maintain my relationship with those of you who were interested in reading it. I also wanted to continue discussion of the issues described in the sub-heading above, in addition to creating an information resource both for myself and others. However, I knew that this would be a tall order for someone with such limited energy resources – and so it has proved.
Clearly, I cannot carry on over-stretching myself in this way so I’ve had to come up with Plan B. I am not going to terminate the blog but I will only write on an ad hoc basis as and when I have something important arising from my work regarding the treatment of ME patients or other significant event. That work has ground to a complete halt recently because I have overloaded myself and, in so doing, probably damaged my health even further. It is the same story for most campaigners who have this illness which is why it is so hard for any of us to bring about change. Any successful campaign has to be sustainable by its activists but by its very nature, ME inhibits real progress.
I am feeling slightly better now and recovering to a more “normal” level. I will take the next few weeks to review my situation in terms of campaigning, writing and pursuing my much-neglected academic work. I greatly value my relationship with all of you who have taken the trouble to read my posts, whether it is as a one-off or on a regular basis. Revealing personal information about myself does not come easily and occasionally I go into a complete meltdown about how much I have said. However, if I don’t do it then I cannot expect others who do not have experience of this illness to understand any of the challenges which I, and so many others, face on a daily basis.
Some bloggers/campaigners avoid this extra stress factor by remaining anonymous and, although I completely understand their reasons for doing so, I think that this reduces the impact of the message. No matter how difficult it is, I believe that being accountable for what I say is an integral part of the process; nevertheless, in my darkest moments, it is terrifying.
**************************************
For the time being I’m going to accept that I need to stop writing and concentrate on doing whatever else I can to bring about change. It’s been a very difficult decision but I think it’s a no-brainer. In the meantime, I can be contacted via Facebook, Twitter, LinkedIn or Google+.
I wish you the best 2013 that you can possibly have. Thank you for reading past, present and (hopefully) future posts.
A time to dance, a time to weep: reflections on a winter’s day
Yesterday was a strange and difficult day. I had planned to be spending time with my inspirational classmates from the 2011-12 LLM (Masters in Law) course at Queen Mary, University of London, celebrating their graduation. Instead I was at the funeral of a member of my extended family in the bitterly cold and foggy East Anglian countryside. Life’s like that.
The last few weeks have been eventful and taxing in a way that I had not anticipated. As John Lennon said – life is what happens when you’re busy making other plans. My other plans consisted of writing my next piece for this blog and preparing for the inevitable (for me) stress of the Christmas/New Year season. Life, however, had other plans of its own. Dealing with the unexpected is often hard for many people. If you live, as I do, with the illness ME, it pretty much screws you completely.
I have had no resources left to write the post(s) which I had planned but I cannot lay this year to rest without thanking you for reading this blog. I plan to continue working and writing as best I can when the New Year gets under way and hopefully I have recovered a little from the events of the last few weeks.
I feel overwhelmingly frustrated by the constraints imposed by my health problems; however, whilst I must accept the necessity of managing my health on a mundane day-to-day basis, I want to avoid focussing on that and concentrate instead on what I hope to do in the future. Much of that revolves around my very slow-cooking plans for practical awareness-raising of the mistreatment of ME patients. However, there will be other subjects too – because life is not a single-issue campaign: hence the sub-title of this blog. I cannot achieve nearly as much work as I would like nor update the blog nearly often enough but there will be more work and new posts as and when I am able.
So I wish you a joyous and peaceful festive season – whoever you are, wherever you are and whatever your religion or belief system. For many people, this season can be a difficult and lonely time, in which case I want to say that I will be thinking of you particularly, even though I may not know you personally.
Thank you for reading this. I hope to meet you again in 2013.
“A time to dance, a time to weep”: http://www.youtube.com/watch?v=fHvf20Y6eoM.
